Download App
Download App
 Doctors for Male Hypogonadism
Doctors for Male Hypogonadism  OTC Medicines for Male Hypogonadism
OTC Medicines for Male Hypogonadism


What is Male Hypogonadism?
Male hypogonadism is a condition characterised by a deficiency in testosterone levels (the hormone that plays the main role in the growth and development of males during puberty), as the body is not able to produce it in sufficient quantities. This condition can have a great impact on the quality of life of the affected. Besides being a sex hormone, testosterone is considered critical for cognitive and body functions (which includes the functioning of the brain and metabolic and vascular systems) and development.
Hypogonadism is of two types, i.e., primary (in the testicles) and secondary (in the hypothalamus or pituitary gland).
What are the main signs and symptoms?
The common signs and symptoms of hypogonadism include
- Anaemia
- Muscle wasting
- Reduced bone mass or bone mineral density or osteoporosis
- Abdominal fat
- Hot flushes
- Decreased body hair
- Delayed epiphyseal closure
- Gynaecomastia
- Sexual dysfunction, including
- Erectile dysfunction
- Reduced energy, stamina, libido, penile sensation, or sperm count
- Difficulty attaining orgasm
- Small testes
- Depressed mood or increased irritability
- Concentration difficulty
- Changes in cholesterol levels
What are the main causes?
The main causes of primary hypogonadism are
- Old age
- Klinefelter's syndrome
- Mumps orchitis
- Haemochromatosis
- Injured or undescended testicles
- Cancer treatment including chemotherapy or radiation therapy
The main causes of secondary hypogonadism are
- Obesity
- Disorders of the pituitary gland
- Stress-induced hypercortisolism
- HIV/AIDS
- Kallmann syndrome
- Diseases which includes tuberculosis, sarcoidosis, histiocytosis
- Medications, such as opiate pain drugs and hormones
How is it diagnosed and treated?
The diagnosis is made by the physician mainly based on the symptoms, and the following tests are advised:
- Hormone testing
- Serum testosterone or free testosterone
- Serum luteinizing hormone (LH) and follicle stimulating hormone (FSH) for secondary hypogonadism
- Semen analysis
- Pituitary imaging
- Testicular biopsy
- Genetic studies
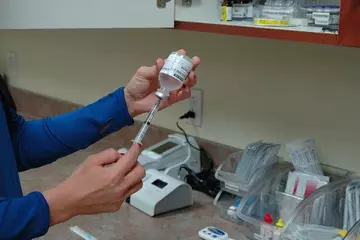
The first line of treatment is testosterone replacement therapy, which should provide 300-800 ng/dL of testosterone. It can be in the form of:
- A transdermal patch that delivers testosterone over a 24-hour period continuously.
- Buccal testosterone tablets, which are used as pulsatile release of testosterone.
- An implantable pellet, which is surgically implanted intended for slow release.
- Topical gel, which is used for longer-lasting elevations in serum testosterone.
- Intramuscular injections are used for prolonged absorption, which are suspended in oil.
- Oral testosterone tablets, currently not available in India.