Download App
Download App
 Doctors for Aortic dissection
Doctors for Aortic dissection 
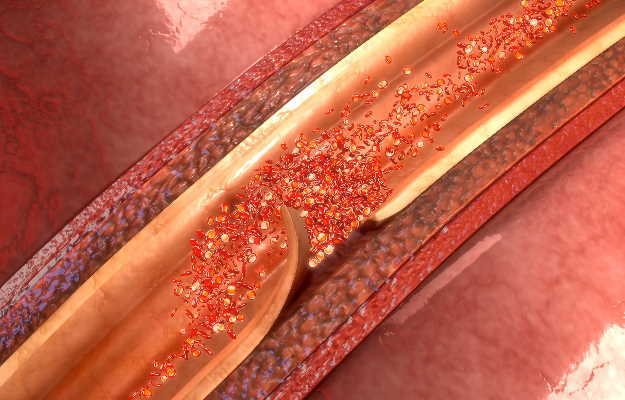
An aortic dissection is a disruption in the wall of the aorta due to intramural bleeding. This dissection results in the separation of the layers of the aortic wall, to form a true and false blood column or lumen.
The aorta is the largest blood vessel in the human body. This artery performs the vital function of carrying blood from the heart, and through the chest and the abdomen. The
arteries that branch off from the aorta supply all the major parts of the body.
Uncontrolled hypertension, cholesterol plaque build-up in the arteries (atherosclerosis), an aortic aneurysm (the blood vessel becomes weak and bulges in places), a heart valve defect and birth defect (aortic coarctation) are some of the risk factors for an aortic dissection.
An aortic dissection is one of the most commonly occurring emergencies affecting the aorta. An aortic dissection is more likely to occur in males as compared to females (nearly 70% of cases of aortic dissection are seen in men). The age group that is most affected is 50-70 years.
In terms of types, an aortic dissection can be acute, subacute or chronic.
1) Acute aortic dissection: Less than 14 days since the disease onset
2) Subacute aortic dissection: 15-90 days since the disease onset
3) Chronic aortic dissection: More than 90 days since the onset of the aortic dissection.
Read on to know more about aortic dissection, what causes it, its symptoms, how it can affect the patient’s health, its diagnosis, treatment and prevention.