Before the surgery:
You will be asked to change into a hospital gown and will be administered with a blood thinner injection to reduce blood clots during surgery and an antibiotic injection. You will also be provided with special leg stockings to reduce the chances of blood clots. An anaesthetist will discuss the anaesthesia and other pain management options with you. The procedure is generally carried out under general anaesthesia (the person is put to sleep).
Before the surgery, a tube will be introduced into your stomach through your nose (nasogastric tube) it is used for nutritional support and remove any excess fluids from stomach. An intravenous drip will be placed to give you fluids to prevent dehydration. A catheter will be inserted into your bladder to track the urine output. These tubes will be removed a few days after the surgery.
Broadly, nephrectomy can be performed using two surgical approaches:
Conventional open nephrectomy
The treatment of choice for kidney cancer that has not spread (localised) and for irreversible kidney damage is open nephrectomy.
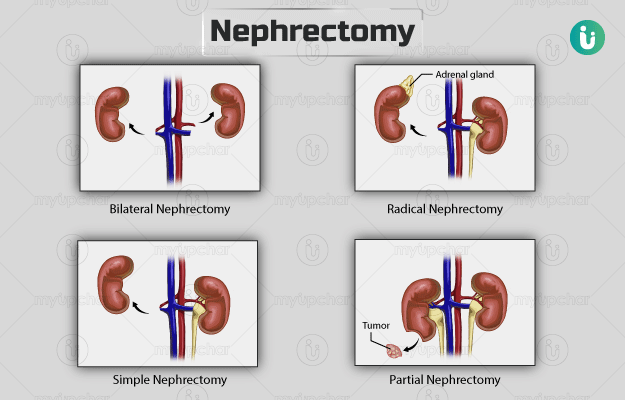
Simple nephrectomy:
- You will be made to lie on your side bent at the waist on an angled table if the surgery is performed from the side to give better access to the kidney.
- A surgeon will cut your skin and muscle and, If required, remove some region of your ribs to access your kidney.
- He/she will then move aside the nearby organs.
- The surgeon will tie up and cut the blood vessels of your kidney and ureter and gently lift y the affected kidney out of your body.
- Finally, the surgeon will suture the lower layers of the incision. The upper layer may be either sutured or stapled.
Radical nephrectomy:
-
The procedure for radical nephrectomy is largely similar to the one described above. However, a larger incision will be made across the front of your abdomen that may extend to the base of your chest. Here, the kidney and neighbouring lymph nodes and adrenal glands are removed.
The procedure may take one to three hours to complete and may require a hospital stay of five to seven days.
Laparoscopic nephrectomy:
This procedure can be performed using a transperitoneal (from the front side of the abdomen) or retroperitoneal (from the backside of the abdomen) approach.
- In the transperitoneal method, the surgeon will make an incision on your abdomen and inflate your abdomen with carbon dioxide for better visibility of your organs. He/she will then make three to four more cuts in your abdomen, to insert instruments for the surgery,
- In the retroperitoneal method, the surgeon will make a small cut on your back, and push a small balloon in to create space. The balloon will be removed, and carbon dioxide will be introduced to fill the space. Thereafter, two or three small incisions will be made in your back for other instruments.
- Through the openings, the surgeon will insert a laparoscope, which is a thin tube with a light and camera on the end in your abdomen. The procedure is facilitated by pictures received from the camera that the surgeon can use to visualise the kidneys and surrounding tissues.
- Using the instruments, the surgeon will dissect your affected kidney from the surrounding tissues and blood vessels and place it in a small bag, which is removed by widening one of the incisions. Alternately, the surgeon will break down your affected kidney into pieces in the bag and then removed through one of the incisions.
- Finally, the surgeon will close the incisions with clips or absorbable stitches that disappear within two to three weeks. You may be given a local anaesthetic to relieve pain.
- The entire procedure takes one to three hours until complete. You will likely be discharged after three days.
After your surgery, you will be moved to the recovery room until the effect of anaesthesia wears off. Then, you will be shifted to the ward.
You will have:
- An oxygen mask that gives you oxygen for the initial one or two days.
- A drain at the wound site to drain fluids collected after the operation.
- A dressing placed on your sutured openings.
Your temperature, blood pressure, pulse, and oxygen levels will be frequently checked. You will wear the support stockings on your legs to prevent blood clots from forming. You may receive medications to avoid blood clots and for pain. You will be encouraged to mobilise as it reduces the formation of blood clot and chest infection. You should be able to have a light meal the day after surgery to initiate normal bowel movements that may be sluggish initially.
Discharge from hospital:
- You will be discharged only after you eat, drink, resume bowel movement, and walk independently.
- Pain medicines will be prescribed to you.
- You will be taught to administer blood clotting medications to yourself before discharge, which you may be asked to continue for about 28 days.



 Download App
Download App