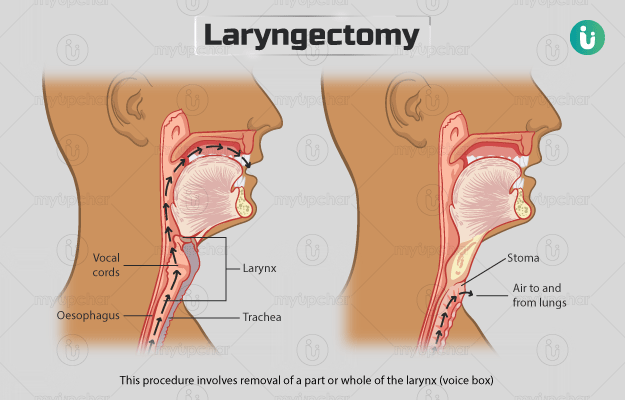
A laryngectomy may be total or partial and the larynx resection (removal) itself can take one to two hours. The larynx, which is connected to the upper part of the trachea (windpipe) allows the passage of air through it, into the lungs.
In a total laryngectomy, the larynx is fully removed, and the airway is blocked. Hence, a separate permanent stoma (opening) is made, and a tracheostomy tube is inserted.
In a partial laryngectomy or hemilaryngectomy, less tissue is removed, and efforts are made to keep the anatomy and function of the larynx maintained. The tracheostomy tube is eventually removed in this type of laryngectomy.
The procedure of a total laryngectomy is:
- A doctor will place a urinary catheter in your bladder to drain urine.
- An intravenous (IV) line will be placed in your arm to provide fluids.
- After giving general anaesthesia (to put you to sleep during the procedure), an artificial tube will be inserted into your windpipe through your neck (intubation) so that you can breathe while your natural airway is compromised.
- Following this, the surgeon will do a laryngoscopy (using a small device used to check the larynx and throat) to check the extent of cancer. A laryngoscopy also helps the surgeon to determine whether the surrounding structures can be surgically removed or not.
- Next, the surgeon will make an incision (cut) on your neck. In case you have an existing tracheostomy, the opening for the tracheostomy will be incorporated into the cut.
- The surgeon will extend the incision deeper to expose the underlying organs, nerves, and blood vessels.
- He/she will remove other cancerous structures surrounding the larynx and then the whole larynx itself.
- Once the larynx has been removed, the surgeon will suture the cut. However, before that he/she will create a permanent stoma (opening) in your neck and insert a tracheostomy tube through it. The end of the windpipe that was originally connected to the larynx will now be attached to this stoma at the base of your neck, enabling you to breathe.
- In the end, the surgeon will place drains near the wound to drain any fluid that collects after the procedure.
A partial laryngectomy may be carried out through the oral opening or through a cut made over the neck. The hole (tracheostoma) made for surgery is temporary in most partial laryngectomy cases. A part of the vocal cord is preserved in most cases so that you can still speak after the surgery.
During the surgery, the surgeon also examines and may remove some of your lymph nodes if needed. This is considered a major surgery which lowers the chance of cancer recurrence.
Sometimes, you may also be given radiation treatment after the surgery. Treatment is usually given one day at a time and does not require long hospital stays by itself.
You can expect the following after the surgery:
- You will have an IV line and catheter in place for a while.
- Pain relief medicines will also be administered to reduce discomfort.
- During the first few days after surgery, you will be fed by a tube that goes into your stomach through your nose, neck or through the abdomen. This tube is removed in one or two weeks if wound healing is satisfactory.
- The tracheostomy tube will be kept in place to prevent the stoma from closing.
- The hospital staff will initially clean the opening through which you are going to breathe (stoma), and in a few days, you will be trained in keeping it clean.
- It is difficult to talk in the days following surgery, and you will be given a notepad or whiteboard to communicate.
- An electronic device may be placed under your tongue or near your neck and, later, a special valve may be placed between your gullet and windpipe, which will allow sound to come out of your mouth, thus allowing you to communicate.
- You will be closely monitored by a speech pathologist to help you learn the new ways of communication and choose one that suits you the best.
- You will stay in the hospital for up to 14 days after your surgery.



 Download App
Download App